
By Gerald McGlothlin
In 2020, the United States faced the shock of a new pandemic — but also a baffling medical mystery: the disappearance of the seasonal flu. While COVID-19 cases dominated headlines and hospital beds, flu diagnoses plummeted to “too low to estimate,” according to the Centers for Disease Control and Prevention, with later estimates at a mere 2000.
That’s not just a statistical anomaly — it’s a statistical impossibility. From an estimated 48 million cases in 2019–2020, the flu dropped to 2000 cases, statistically zero, in 2020–2021, amounting to a 99.999998% decrease — or put another way, a nearly 10 million percent drop. In the realm of infectious disease, that kind of disappearance doesn’t happen without a force far greater than a virus. In this case, that force may have been government incentives, diagnostic bias, and political opportunity.
Side-by-Side Comparison: Flu vs. COVID-19 (and Total Deaths)
Here is a year-by-year comparison of flu and COVID-19 cases in the U.S., alongside total recorded deaths from all causes:
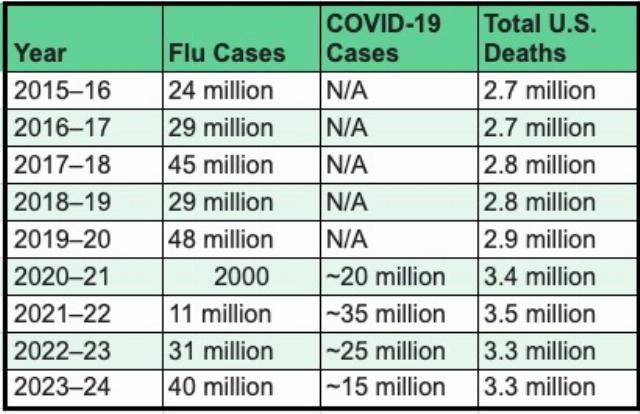
If mask mandates, social distancing, and lockdowns truly drove flu cases to extinction in 2020, why did COVID-19 — transmitted in much the same way — surge to 20 million cases that same year? It’s a paradox that challenges the public narrative.
Under the CARES Act, hospitals received a 20% bonus payment from Medicare for every inpatient COVID-19 case. Emergency relief funds, FEMA reimbursements, and hazard pay followed. In some cases, physicians were allowed to list COVID-19 as the cause of death even without a lab-confirmed test — if the diagnosis was “presumed.”
Dr. Scott Jensen, a physician and former Minnesota senator, explained in a 2020 interview, a special incentive given to hospitals: “Right now, Medicare has determined that if you have a COVID-19 admission to the hospital, you get $13,000. If that patient goes on a ventilator, you get $39,000.”
Even without malice, human systems respond to incentives. Hospitals, stretched to the brink and under administrative pressure, had clear financial reasons to code ambiguously respiratory cases such as COVID. The result? Flu diagnoses plummeted; COVID statistics ballooned.
Historians may look back and label 2020 a “perfect storm” convergence of viral emergence, bureaucratic overreach, financial opportunism, and media-driven fear. The COVID-19 diagnosis wasn’t always wrong — but it was often preferred, because it brought funding, media coverage, and regulatory attention.
Into this maelstrom stepped the Biden campaign — and later, the Biden administration. From their perspective, the pandemic was not just a crisis; it was an opportunity to centralize authority, impose sweeping mandates, and frame their political opponents as anti-science.
Vaccine passports, mask mandates, and “non-essential business” closures were implemented with minimal congressional oversight. Unelected bureaucrats effectively became lawgivers overnight. And with a compliant media ecosystem, anyone questioning the sudden disappearance of the flu — or the overreporting of COVID — was dismissed as a conspiracy theorist.
But as total U.S. deaths jumped from 2.9 million in 2019 to 3.4 million in 2020, and yet flu deaths were negligible, the public was expected to suspend disbelief. It was COVID. Everything was COVID. Even if someone had flu-like symptoms, pneumonia, or comorbidities, the incentives were aligned to make it COVID.